{kind=link}
Parliamentary Office for the Assessment of Scientific and Technological Choices (OPECST)* Hearing of 25-09-2019
presented at the National Assembly by
Professor Jean Costentin Member of the National Academies of Medicine and of Pharmacy
co-authors:
Professor Jean-Pierre Goullé, Titular Member of the National Academies of Medicine and of Pharmacy,
Professor Jean-Claude Alvarez, Corresponding Member of the National Academy of Pharmacy.

Legalization of “therapeutic cannabis”
First of all, let us be surprised at the exceptional procedures implemented to grant a substance medicinal status (media campaign, policy intervention, creation of a special study committee (CSST)**, which provides elements of conclusion before having the data to be collected.
As with any medicine, cannabis (already qualified as therapeutic before the data that must decide on it are collected) must be evaluated (with perfectly defined active ingredients, precise medical indications and, as a priority, the determination of their benefit-risk relationships; all essential elements for obtaining a possible marketing authorization (AMM). It should be reminded that four medicines, derived from synthetic cannabinoids and from a pure cannabis extract (cannabidiol or CBD) are currently authorized for certain diseases with specific medical prescription conditions:
1 – Tetrahydrocannabinol (THC) obtained by synthesis (Dronabinol / Marinol®) and a synthetic derivative of this THC (Nabilone / Cesamet®) may be prescribed to treat nausea and vomiting due to cancer chemotherapy and to stimulate appetite. Marinol® and Cesamet® are subject to a temporary authorisation for use (ATU) regime. It should be noted that the annual requests for patients to be treated are limited to a few hundreds.
2 – Cannabidiol (CBD) or Epidyolex® is authorized as adjuvant therapy in the context of an ATU for the management of certain rare and severe forms of epilepsy in children.
3 – The combination of THC and CBD in Sativex®, in the form of aerosols for oral sprays, obtained in 2014 a marketing authorization for “the symptomatic adjunctive treatment of manifestations of spasticity, related to multiple sclerosis, in patients insufficiently relieved by reference antispastic treatments”. The medical service rendered (SMR) for Sativex® was considered “insignificant” by the National Medicament Safety Agency; its reimbursement rate was set at 15% due to excessive pricing. In the absence of a price-agreement, the medicine is not currently marketed in France (this was presented by some in 2014 as a major, essential drug…).
The world pharmaceutical industry, in search of analgesic and anti-inflammatory medicines, has invested considerable sums to design more than a hundred cannabinoids; they have all shown adverse benefit-risk ratios that do not allow them to qualify as medicines. These and other cannabinoids (over 200) are currently available on the drug market, all of which are diverted for exclusively addictive purposes.
“Therapeutic cannabis”
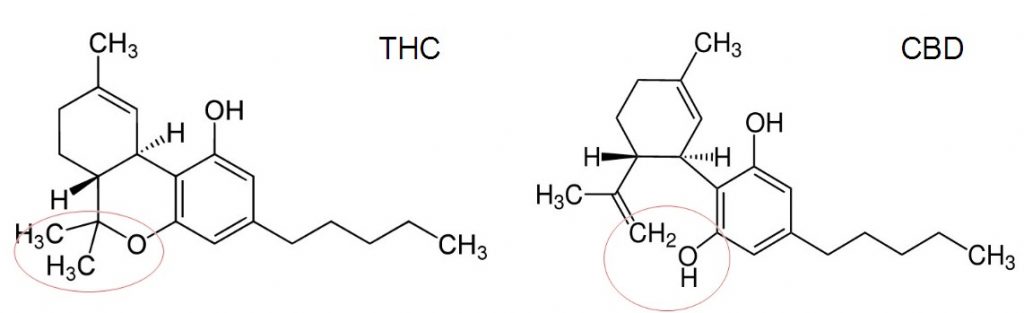
This term is a real misuse of language. The “therapeutic cannabis” misleads patients’ expectations by posing as “therapeutic”. Such a name refers to the plant, the whole plant, which has hundreds of components and which, unlike the five cannabinoids mentioned above, does not meet the criteria defining a medicine. Indeed, the status of “medicinal product” is the result of a rigorous control, risk analysis and validation process that leads to the granting of a Marketing Authorization (AMM). Any “medical” or “therapeutic” designation applied to a product that has not followed this long regulatory process is abusive and illegal. In the case of cannabis, the plant (the whole plant) contains, along with other compounds, about 100 cannabinoids chemically related to THC. Among them, the tetrahydrocannabinol (THC) and cannabidiol (CBD) are dominant. It should be mentioned that the plant’s modest pharmacological effects, but above all its main harms, foremost among which is the risk of addiction, led to its withdrawal from the French pharmacopoeia in 1953. Today, with the considerable increase in THC levels in cultivated cannabis, this risk of addiction has increased significantly.
In the claimed indications, there are real medicines available that have a specificity of action; an intensity of action at least equal to and generally much greater than that of cannabinoids; a pharmacokinetics that is free of accumulation in the body, with a very long duration of action, that does not induce medicinal interactions by action on glycoprotein P (Gp P), that is not addictive, and that does not accumulate multiple adverse effects.
The target of cannabinoids are the CB1 receptors; they are the most numerous of all brain receptors. They are ubiquitous and thus simultaneously affect a multitude of functions, burying the one we would like to solicit in the noise of a hundred others, useless or even deleterious.
Legalization of “recreational cannabis
Preliminary remark: All countries that have legalized cannabis for recreational purposes (some states in the United States, Canada, etc.) have previously endorsed it as a medicine.
For obvious health reasons, cannabis is dangerous to health, as are tobacco and alcohol. At a time when the aim is to stop smoking and reduce alcohol consumption, it is not responsible to consider the recreational use of cannabis.
Alcohol, tobacco and illicit drugs are responsible for 130,000 deaths annually (355 deaths per day) and their annual social cost amounts to 249 billion euros (Kopp P. Le coût social des drogues en France. Observatoire français des drogues et toxicomanies, note 2015-04, 10pp). This social cost takes into account the cost of lost lives, loss of quality of life, loss of production and the effect on well-being. The annual individual social costs for problematic users of alcohol, tobacco and illicit drugs (mainly cannabis) are respectively 32,000 – 9,000 – 29,000 euros. The direct cost of drugs (cost of care, pension savings, prevention and repression, taxation) to public finances is considerable; €14.8 billion for tobacco, €4.9 billion for alcohol and €2.4 billion for illicit drugs, for a total of €22.1 billion, or 1% of GDP. This direct cost accounts for 5.5% of public spending, which amounts to 380 billion. Contrary to popular belief, taxes levied on alcohol and tobacco only cover 37% and 40% respectively of the cost of care caused by the pathologies related to their consumption. Our country already pays a very heavy price for these two licit drugs, so in terms of health, our society would bear the very heavy responsibility of adding recreational cannabis to it.
The harms of cannabis to the brain, particularly through its THC, are becoming increasingly well known, as scientific and epidemiological data continue to accumulate:
1. Cannabis use from adolescence to 24 years of age is contemporary with the period of brain maturation; it is a critical period of neuropsychological development and high vulnerability to addictions.
2. THC induces addiction (or drug dependence), which affects nearly 20% of those who have experienced it (in France there are 1,400,000 regular users; including 700,000 daily and multi-daily users; 7.4% of 17-year-olds have problematic cannabis use (ESCAPAD*** 2017 survey).
3. THC persists in the brain and body fats for days and even weeks, so its effects are very persistent; it is “a very slow drug”.
4. It disrupts awakening, attention, short-term memory (without which long-term memory cannot be formed); this causes serious cognitive and educational disturbances.
5. It produces an intoxication, quite comparable to that caused by alcohol; with which it gives rise to mutual potentiation; thus, the encounter of cannabis and alcohol multiplies by 14 the risk of being responsible for a fatal road accident (narcotic investigation and fatal accidents). In 2017, 23% of subjects killed in road traffic accidents tested positive for narcotics, 90% of whom were cannabis.
6. It induces delusional and hallucinatory disorders, such as those experienced during madness (schizophrenia).
7. It is at the origin, in acute, of possible anxiety attacks, but more often of an anxiolytic effect, which incites the anxious to use it and soon to abuse it, developing a tolerance, which then makes an anxiety reappear much more intense than it was initially.
8. THC is perceived during its first uses by a depressed subject as an antidepressant, which encourages him to use it, then to abuse it, until the disappearing effect (tolerance) causes an intense depression to reappear, with a suicide risk in ambush.
9. At the rate that the effects of THC are diminishing (tolerance), the cannabinophil often adds other drugs to it, creating polyaddiction.
10. THC can trigger cannabic psychosis, which regresses only under antipsychotic treatment; it will not reappear if the subject never uses cannabis again.
11. THC can install de novo, or decompensate, a vulnerability to schizophrenia, and thus reveals this serious condition, from which there is no cure. It induces resistance to the treatments (antipsychotics) that are given to it.
Cannabis, through its THC, has deleterious effects on other functions and organs:
1. Its toxicity is obvious for the body: Acceleration of the heart rate; vasodilation in certain territories; triggering of arteritis of the lower limbs, (which can occur in the young subject, therefore much earlier than those induced by tobacco); in the same register, and with the same precocity, induction of strokes, heart attack. THC is an immunity depressant; it reduces the resistance that the individual can exert to microbial aggressors.
2. THC disrupts growth; at 20 years of age, height is estimated to be on average 10 cm and weight 4 kg less than that observed in adolescents who have not smoked cannabis.
3. THC is concentrated in the testicles, reducing the secretion of the male hormone, testosterone, which in the long run determines a decrease in libido, a certain degree of regression of male sexual characteristics, as well as a decrease in sperm in the seminal fluid. In addition, cannabis is implicated in the occurrence of an aggressive variety of testicular cancer (non-seminoma germinoma).
4. Cannabis is a bad pairing with pregnancy; three out of four women who use it are unable to abstain from it. This shortens the duration of gestation and results in babies being born at a lower weight than would be the case with prematurity alone. The risk of unexplained sudden death is higher in these “cannabis babies”, their psychomotor development is delayed throughout childhood; the frequency of development of attention deficit hyperactivity disorder is increased.
5. Even more serious, through an epigenetic phenomenon, the exposure of subjects of childbearing age to THC transmits to their immediate descendants a strong appetite for all drugs, which will manifest itself as early as adolescence.
Cannabis is therefore clearly dangerous from a health point of view. The countless data accumulated in recent years establish or confirm the multiple dangers to which it exposes its consumers.
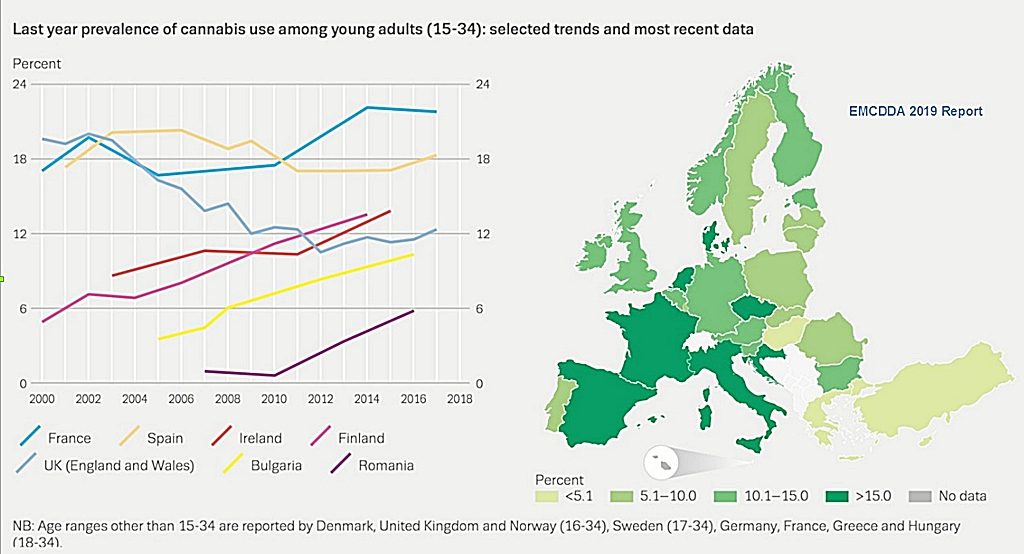
Unfortunately, France is the largest consumer in European countries, with 1,300,000 individuals in France having become regular users; a considerable number given its status as an illegal drug.
There is no way to get THC-dependent subjects to give up this drug, it should be remembered that 7.4% of 17-year-old adolescents have problematic cannabis use.
The experience of other countries that have legalized it already shows a number of negative effects. We even have several studies with figures from the United States concerning:
– The trivialization of cannabis use: a very large study, conducted in 39 American states, involving 118,500 subjects, over three periods: 1991-1992, 2001-2002 and 2012-2013, assessed the impact of authorizing the use of cannabis for medical purposes on its illicit use. Over the entire period of more than 20 years, between 1991-1992 and 2012-2013: the illicit use of cannabis in the population has increased overall in all States, but it has increased more in the 15 States that have authorized its use for therapeutic purposes (the percentage of use in these States has increased from 5.55% to 9.15%, or +3.6%), while in the 24 States where the drug has retained its illicit status, its consumption has increased less (from 4.5% to 6.7% or +2.2%);
– The increase in the number of subjects with addiction: the results of the previous study show, based on demographic trends in the United States, that the authorization of cannabis use for medical purposes is responsible for an additional number of illicit users or those with addiction to this drug, estimated at 1.1 million and 500,000 individuals respectively.
– The increase in accidents: Studies in Colorado and Washington State, which have legalized cannabis use, show a significant increase in driving under the influence of cannabis. In Washington State, in 2014, the number of cannabis-impaired drivers killed in a fatal traffic accident more than doubled after the legalization of the drug, reaching 17% according to official statistics. In Colorado, in 2015, 21% of drivers killed tested positive for cannabis. Deaths related to this drug increased by 48% on average over three years (2013-2015), compared to the period before the legalization of cannabis for recreational use (2010-2012), during which the total number of road deaths increased by 11%.
Some argue that France’s repressive policy against drug use for more than 40 years is a bitter failure. There is absolutely no question of repressive failure, because in France, there is no repression for the simple use of cannabis, it is a “fake news” put forward by the pro-legalizers. In France, the framework for the policy to combat illicit drugs was initially established by the 1970 Act (Act No. 70-1320 of 31 December 1970 on health measures to combat drug abuse and to combat trafficking in and illicit use of poisonous substances). This French law seems repressive, but it is not applied at all both for simple use and for trafficking, as shown by the European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) in its report published in 2017. It shows that the prison sentences for offering one kilogram (1 kg) of heroin or cannabis vary considerably among the 25 countries participating in this survey. For example, in Greece, the country with the highest penalties, the offer of one kg of heroin leads to a median sentence of 20 years’ imprisonment and the offer of one kg of cannabis leads to a median sentence of 10 years’ imprisonment (see figure). At the other end of the scale are the two most tolerant countries, the Netherlands and France, for which the offer of one kg of heroin leads to a median sentence of 1 year and 2 years respectively. As for the offer of one kg of cannabis, the penalty may be suspended in these two countries, it is not shown in the figure.
In addition, French law has been deeply relaxed by the Taubira law and its implementing decrees. Thus, the 2014 Act (Act No. 2014-896 of 15 August 2014 on the individualization of sentences and strengthening the effectiveness of criminal sanctions) introduces new provisions such as the use of sentence adjustment, depending on the circumstances of the offence, the personality of the offender, his material, family and social situation. A decree implementing this law, published in October 2015, introduced the criminal transaction for minor offences punishable by a maximum of one year’s imprisonment, including the simple use of narcotics. With the prior agreement of the Prosecutor, it consists of the immediate payment of a fine that extinguishes the public action. The 1970 law was not applied for the simple use of cannabis and the 2014 law with its 2015 implementing decree rendered it definitively ineffective. However, it is the ineffectiveness of the repressive 1970 law, according to some, that is responsible for the failure of illicit drug policy in our country and in particular for the very high consumption of cannabis. At least this is the argument systematically put forward to demand the depenalization/legalization of this drug, even of all drugs.
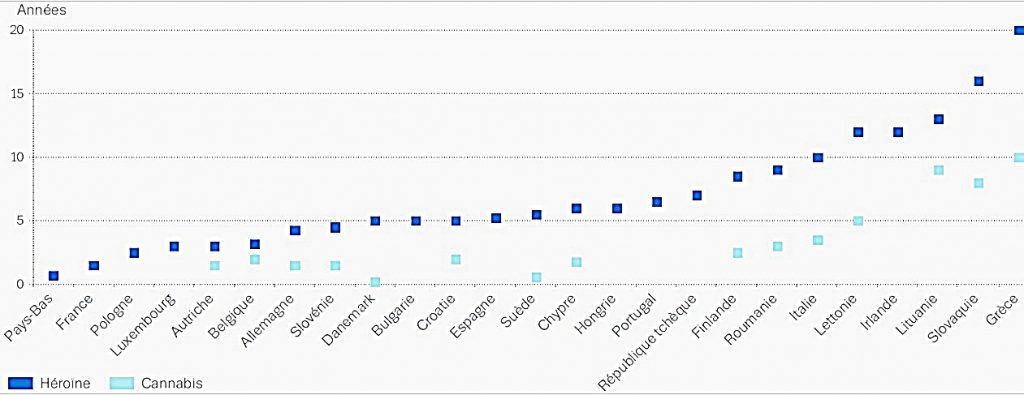
Figure: Planned median sentences based on the opinions of a sample of lawyers in each country and involving non-recidivist perpetrators with no connection to organized crime. When the sentence can be suspended, the median sentence is not presented (Source: EMCDDA, June 2017).
As for the idea of affirming that state legalization would make it possible to control the quality and power of cannabis, this is utopian. The regular user will smoke twice as much to experience the same effects if the THC content is half as low, the only medical and psychological help that can be provided is medical withdrawal. It should be reminded that the control of THC content was one of the objectives of legalization in Canada and that after 18 months, the share of state cannabis is only 40%, the illicit market having retained 60% of the market (cannabis with a higher THC content and lower price).
It is important to mention the extreme vulnerability of adolescents and young adults up to the age of 24 (end of the period of brain maturation) to drugs (alcohol, tobacco, cannabis), which justifies particularly strong information and prevention actions at an early stage, which are not carried out in France. In its 2017 report, the EMCDDA gives our country a red card in the field of prevention. He denounces a serious lack of information on drugs in schools. In particular, it notes the lack of targeted interventions in school programmes (rating 1 out of 5), unlike what is achieved on average in our European neighbours (rating 3 out of 5). In addition, reducing vulnerability factors at this stage of life is essential to limit the risk of exposure to and damage from licit and illicit drugs. In the case of addiction, appropriate early medical care should be provided by providing integrated treatment (addictions – psychiatric disorders – personality disorders). The implementation of an ambitious policy of information and prevention on licit and illicit drugs among adolescents is essential, in particular with the support of targeted teaching in educational programmes from primary school, then in middle school, high school and university. Their inadequacy is a serious lack and a threat to adolescents. Information and prevention must therefore be rapidly integrated into educational programmes, but also the role of parents and carers in providing early information and prevention must be strengthened in order to protect the health of our adolescents.
Short-form references
- Nawrot TS, Perez L, Künzli N, et al. Public health importance of triggers of myocardial infarction: a comparative risk assessment. Lancet, 2011.
- Szutorisz H, Hurd Y. Epigenetic effects of cannabis exposure. Biological Psychiatry, 2016.
- Gobbi G, Atkin T, Zytynski T, et al. Association of Cannabis Use in Adolescence and Risk of Depression, Anxiety, and Suicidality in Young Adulthood: A Systematic Review and Meta-analysis. JAMA Psychiatry, 2019.
- Krebs MO, Kebir O, Jay TM. Exposure to cannabinoids can lead to persistent cognitive and psychiatric disorders. Eur J Pain, 2019.
- Andréasson S, Allebeck P, Engström A et al. Cannabis and Schizophrenia. A Longitudinal Study of Swedish Conscripts. Lancet, 1987.
- Zammit P, Allibeck P, Andréasson S et al. Self-Reported Cannabis Use as a Risk Factor for Schizophrenia in Swedish Conscripts of 1969; Historical Cohort Study. Brit Med J, 2001.
- Arsenault L, Cannon M, Poulton R et al. Cannabis Use in Adolescence and Risk for Adult Psychosis: Longitudinal Prospective Study. Brit Med J, 2002.
- Bilan définitif de l’accidentalité routière 2017, Observatoire national interministériel de la sécurité routière.
- Aldington S, Harwood M, Cox B, et al. Cannabis and Respiratory Disease Research Group. Cannabis use and risk of lung cancer: a case-control study. Eur Respir J. 2008.
(*) OPECST : Office Parlementaire d’Evaluation des Choix Scientifiques et Techniques. The co-authors are the Professors J.P. Goullé and J.C. Alvarez toxicologists and the Professor J. Costentin, pharmacologist. The illustrations were added except for the “Figure“.
(**) CSST : Comité Scientifique Spécialisé Temporaire – Temporary Specialized Scientific Committee
(***) ESCAPAD : Enquête sur la Santé et les Consommations lors de l’Appel de Préparation à la Défense – Survey on Health and Consumption During the Call for Defence Preparation.
oOo